Dynamic or Static Stretching? Which is best?
There has been an ongoing debate over the last decade as to what is the best type of stretching for sports performance and injury prevention: dynamic or static stretching?
A definition of both dynamic and static stretching is required to answer this question:
[one_half] Static stretching is used to stretch muscles while the body is at rest. It is composed of various techniques that generally lengthen a muscle to an elongated position (to the point of discomfort), which are held for a period of 15 seconds to 2 minutes. For example, a static hamstring stretch as seen below:
 [/one_half] [one_half_last] Dynamic stretching on the other hand uses movement or momentum of the limb or trunk to move the muscle between its extremes of range. It is a controlled movement and should not be vigorous or bouncy at the end of range. For example, a dynamic hamstring leg swing as seen below:
[/one_half] [one_half_last] Dynamic stretching on the other hand uses movement or momentum of the limb or trunk to move the muscle between its extremes of range. It is a controlled movement and should not be vigorous or bouncy at the end of range. For example, a dynamic hamstring leg swing as seen below:
 [/one_half_last]
[/one_half_last]
Sports Performance
A recent review of the current research pertaining to pre-exercise static stretching by Simic et al (2013) found that static stretching prior to exercise can actually reduce muscle strength, power and explosive performance. The review included 104 studies on static stretching and concluded that “the usage of static stretching as the sole activity during the warm-up routine should generally be avoided”.
A closer look at this review, however, found the detriments in performance (although statistically significant) to be quite small (between 1.9-5.0%). It is also worth noting that these negative effects are in fact negligible if the stretch was held for less than 45 seconds (which most stretches are) and the negative effects were only short lived, with performance returning back to normal within 5-10 minutes after stretching. The review also further concludes that short static stretching is recommended for activities that involve slower eccentric contractions or sports that require greater ranges of movement. Some examples would include the ability of a goaltender in ice hockey to maximally abduct his/her legs when in a butterfly position, gymnasts performing and holding a split position, wrestling, martial arts, synchronized swimming, figure skating and others. Although some studies have indicated that dynamic stretching provides similar increases in static flexibility as static stretching (Beedle and Mann 2007), other studies have indicated that dynamic stretching is not as effective at increasing static flexibility as static stretching within a single warm-up session (Bandy et al. 1998; O’Sullivan et al. 2009) or with prolonged training (Covert et al. 2010). Hence, it could be important to include static stretching in the warm-up for specific sport flexibility applications.
In the context of dynamic stretching, the literature tends to indicate that greater than 90 seconds of dynamic stretching prior to exercise may significantly enhance performance (Bacurau et al. 2009; Beedle et al. 2008; Bradley et al. 2007; Christensen and Nordstrom 2008; Gelen 2010; Jaggers et al. 2008; Papadopoulos et al. 2005; Samuel et al. 2008; Sekir et al. 2009; Torres et al. 2008; Unick et al. 2005). 10 minutes of dynamic warm-up activities (stretching or aerobic activity) have been reported to result in improvements in shuttle run time, medicine ball throw distance and five step jump distance (McMillian et al. 2006). A study by Hough et al (2009) also demonstrated improvements in performance, with an increase in vertical jump height and quadriceps EMG activity after 7 minutes of dynamic stretching.
Injury Prevention
With respect to the effect of pre-participation static stretching on injury prevention, a limited number of studies of varying quality have shown mixed results for both dynamic or static stretching. A general consensus is that stretching in addition to warm-up does not affect the incidence of overuse injuries. There is limited evidence that pre-participation stretching reduces the incidence of muscle strains but there is clearly a need for further work (McHugh et al 2010). Future studies should use stretching interventions that are effective at decreasing passive resistance to stretch and assess effects on subsequent injury incidence in sports with a high prevalence of muscle strains.
What is the take home message?
To achieve optimal sports performance, the warm-up should be composed of a submaximal intensity aerobic activity followed by large amplitude dynamic stretching and then completed with sport specific dynamic activities. As static stretching can still increase range of motion, it still plays an important role for health-related benefits associated with flexibility and particular sports or activities that necessitate a great increase in static ROM relative to the flexibility of the athlete or patient. However, static stretching should normally not be pursued prior to strength, high speed, explosive or reactive activities, except during sports that require greater ranges of movement (static stretches should be held for no longer than a total of 30 seconds per muscle group). All individuals should include static stretching in their overall fitness and wellness activities for the health and functional benefits associated with increased range of motion and musculotendinous compliance. However, a separate static stretch training workout time or during post-exercise cool-down should be planned independent of other training workouts or competitions to achieve a more permanent change in flexibility for health or performance.
References:
Bacurau RF, Monteiro GA, Ugrinowitsch C, Tricoli V, Cabral LF, Aoki MS (2009) Acute effect of a ballistic and a static stretching exercise bout on flexibility and maximal strength. J Strength Cond Res 23:304–308
Bandy WD, Irion JM, Briggler M (1998) The effect of static stretch and dynamic range of motion training on the flexibility of the hamstring muscles. J Orthop Sports Phys Ther 27:295–300
Beedle BB, Mann CL (2007) A comparison of two warm-ups on joint range of motion. J Strength Cond Res 21:776–779
Behm DG, Chaouachi A. A review of the acute effects of static and dynamic stretching on performance. Eur J Appl Physiol 2011: 111: 2633–2651.
Behm DG, Bambury A, Cahill F, Power K. Effect of acute static stretching on force, balance, reaction time, and movement time. Med Sci Sports Exerc 2004: 36: 1397–1402.
Christensen BK, Nordstrom BJ (2008) The effects of proprioceptive neuromuscular facilitation and dynamic stretching techniques on vertical jump performance. J Strength Cond Res 22:1826–1831
Covert CA, Alexander MP, Petronis JJ, Davis DS (2010) Comparison of ballistic and static stretching on hamstring muscle length using an equal stretching dose. J Strength Cond Res 24(11): 3008–3014
Gelen E (2010) Acute effects of different warm-up methods on sprint, slalom dribbling, and penalty kick performance in soccer players. J Strength Cond Res 24:950–956
Jaggers JR, Swank AM, Frost KL, Lee CD (2008) The acute effects of dynamic and ballistic stretching on vertical jump height, force, and power. J Strength Cond Res 22:1844–1849
McHugh MP, Cosgrave CH. To stretch or not to stretch: the role of stretching in injury prevention and performance. Scand J Med Sci Sports 2010: 20: 169–181.
O’Sullivan K, Murray E, Sainsbury D (2009) The effect of warm-up, static stretching and dynamic stretching on hamstring flexibility in previously injured subjects. BMC Musculoskelet Disord 10:37–42
Papadopoulos G, Siatras T, Kellis S (2005) The effect of static and dynamic stretching exercises on the maximal isokinetic strength of the knee extensors and flexors. Isokinetics Exerc Sci 13:285–291
McMillian DJ, Moore JH, Hatler BS, Taylor DC (2006) Dynamic vs. static-stretching warm up: the effect on power and agility performance. J Strength Cond Res 20:492–499
Samuel MN, Holcomb WR, Guadagnoli MA, Rubley MD, Wallmann H (2008) Acute effects of static and ballistic stretching on measures of strength and power. J Strength Cond Res 22:1422–1428
Sekir U, Arabaci R, Akova B, Kadagan SM (2009) Acute effects of static and dynamic stretching on leg flexor and extensor isokinetic strength in elite women athletes. Scand J Med Sci Sports
Simic L., Sarabon N., Markovic G. Does pre-exercise static stretching inhibit maximal muscular performance? A meta-analytical review Scand J Med Sci Sports 2013: 23: 131–148
Torres EM, Kraemer WJ, Vingren JL, Volek JS, Hatfield DL, Spiering BA, Ho JY, Fragala MS, Thomas GA, Anderson JM, Hakkinen K, Maresh CM (2008) Effects of stretching on upper body muscular performance. J Strength Cond Res 22:1279–1285
Unick J, Kieffer HS, Cheesman W, Feeney A (2005) The acute effects of static and ballistic stretching on vertical jump performance in trained women. J Strength Cond Res 19:206–212
How much can I increase running distance per week and still limit my injuries?
It has often been suggested that the 10% rule was the best amount to increase running distance. But this has been more based on clinical experience then research.
A recent research paper published in the October edition of Journal of Orthopaedic and Sport Physical Therapy attempted to shed light on this topic. They completed a one-year study into 874 novice runners and looked at what was the safe amount of running distance increase without sustaining an injury. At the completion of the study they determined that if you increase running distance weekly by more than 30% over a 1-week period you were more likely to sustain a distance related injury then those who increased less than 10%.
(Distance related injuries are injuries like patellofemoral pain (knee cap pain), iliotibial band syndrome, patellar tendinopathy, gluteus medius injury, greater trochanter bursitis, and tensor fascia lata injuries).
The lowest amount of distance related running injuries came from the group who increased their weekly distance by less than 10%. Caution should be taken not to increase just under 30% for more than a 1-week period (for example, 25% for 4 weeks) as there is a potential to again increase the chance of injury.
So what is your magic number? Unfortunately that may be depended on a number of factors such as age, weight, previous injuries and types of injuries. So if you have any questions about determining the safest way to increase running distance speak to one of your physios at Sydney Stadium Sports Physiotherapy.
References:
Nielsen, Parner, Nohr, Sorensen, Lind, & Rasmussen. (2014). Excessive progression in weekly running distance and risk of running-related injuries: an association which varies according to type of injury. Journal of Orthopaedic and Sports Physiotherapy. 44 (10), 739-748.
Shin Splints: What is it and how can it be treated?
Shin splints is one of the most common reasons for exercise-induced leg pain.
The incidence is as high as 6-16% of all running injuries.
With summer right around the corner further awareness of the possible causes of your leg pain is essential in effective management and prevention.
Shin splints, as it is most commonly called, refers to pain on the inside of the shin bone. It does not imply a specific diagnosis, but rather the presence of pain over the shin. Specific anatomical and pathological differences exist that lead to differential, and more specific, diagnoses.
The pain felt can be due to problems of the muscles, the bone, or the attachment of the muscles to the bone. Therefore based on your specific diagnosis, management and treatment will vary.
For optimal management and recovery, assessment by a physio should be undertaken to ensure an accurate and specific diagnosis. The three main pathologies that can cause shin pain are:
1) Medial tibial stress syndrome:
Medial tibial stress syndrome occurs when overuse causes irritation and microtrauma to the soleus (our deep calf muscle) at the attachment to the shin bone. Repetitive stress can also cause irritation to the tibialis posterior muscle, and inflammation of the periosteum (the connective tissue that covers the bone.) This is what most people are talking about when they refer to ‘shin splints’ as their diagnosis. Patients complain of a diffuse pain along the inside of the shin, which usually decreases with warming up so they are able to complete the rest of their training. However pain returns after finishing training and is worse the next morning.
2) Medial tibial stress fracture:
This is most common in athletes involved in running, jumping and impact sports. The incidence increases if play is on a rigid, unforgiving surface. It results as a continuum from increased bone strain, to stress reaction, to finally a stress fracture. Pain has often developed gradually, and usually correlates with an increase in training. Pain worsens throughout a training session and often is present at rest or a night. There is often a focal pain when palpating the shin bone, and a bone scan or MRI can accurately confirm the fracture (an X-ray will often not show it in the early phase.)
3) Exertional compartment syndromes:
The lower leg has a number of muscle compartments, each enveloped by a thick fascia which has limited flexibility. Increased blood flow to the muscle with exercise causes the muscle to increase in size- hence increasing the pressure within compartments. This can lead to decreased blood flow and tissue perfusion, which in turn causes pain. The athlete complains of an increasing achy pain and tight sensation with exercise, but these symptoms usually have disappeared within a few minutes of rest, and are absent at night. Treatment is initially conservative; with deep massage therapy, dry needling, lowering the heel in a shoe, and reducing exercise load. However if this is unsuccessful, surgical release may be necessary to release the fascia surrounding the compartment, with 80-90% of people being able to return to their previous level of sport.
The foundation of treatment starts with an accurate diagnosis
As evidence to date has still not specifically determined a cause, prevention is difficult; however there have been proposed risk factors. Predisposition factors include abnormal biomechanics, (for example pronated feet) ankle instability, weak soleus or tibialis posterior muscles, stiff ankle joints, inadequate shoes, body mass index, inadequate calcium intake or recent growth spurts. Symptomatic relief, (rest, ice) identification of risk factors and treating the underlying pathology are essential for effective management. Regular calf stretches and releases are integral. Increasing the strength and endurance of the soleus/tibialis posterior, controlling over-pronation, and promoting adequate shock absorption via insoles and new shoes is successful treatment. Committing at least one day per week to a pool/cycling/cross-fit session is shown as effective management of medial tibial stress syndrome and also at decreasing load to reduce the risk of medial tibial stress fractures. Continuing to push through shin pain can have dire effects on not only your sporting performance and event participation, but also cause further damage in the long term. See your physiotherapist for an accurate diagnosis and management to maximise your ability this upcoming running season.
Sitting and Low Back Pain: Is there a right way to sit?
As physiotherapists, we very often get asked “how should I be sitting at work to prevent my back from getting sore”? Low back pain affects around 80% of Australians at some stage in their life, and it is the most common workplace health complaint. With an increasing number of sedentary individuals with back pain within the workplace, there has been a growing interest into the causes of low back pain. Recent research has identified that sitting for long periods could perhaps be a major problem for your lower back health.
To put it simply, people who sit a lot have more lower back pain and earlier disc degeneration (Videman T, Nurminen M, Troup J. 1990). But if the type of work you do requires you to sit for long periods throughout the day, is there a better way to sit? An interesting study by Hedman and Fernie (1997) investigated the mechanical response of human lumbar spines to sustained loading in different sitting postures. Twelve lumbar spines were subjected to constant loading conditions while in either a flexed or extended seated posture. The results of the study revealed that there are greater anterior disc compressive forces and higher disc shear and posterior ligament forces in the flexed seated posture compared with the extended posture. However, regardless of the sitting posture, there was an increase in spinal loading and compression as compared to a standing posture. The authors concluded that the “minimization of disc shear, tolerable levels of ligamentous tension, lower disc loads and a balancing of facet impingement and articular facet forces were found to be characteristics of prolonged erect sitting in this study. Based on these results, one would expect that the extended seated posture would reduce exasperation of tissues as compared to flexed postures.”
So with this information, it would seem that sitting and low back pain are related but sitting with a more erect posture is more favourable for our long term lower back health compared with the flattened, flexed posture. But given that sitting for long periods with any posture results in increased spinal loading, frequent changes in position from sitting to standing is highly recommended in the prevention of low back pain and pathology. Regular changes in position every 45-60 mins is recommended if you are going to be sitting for an extended period during the day.
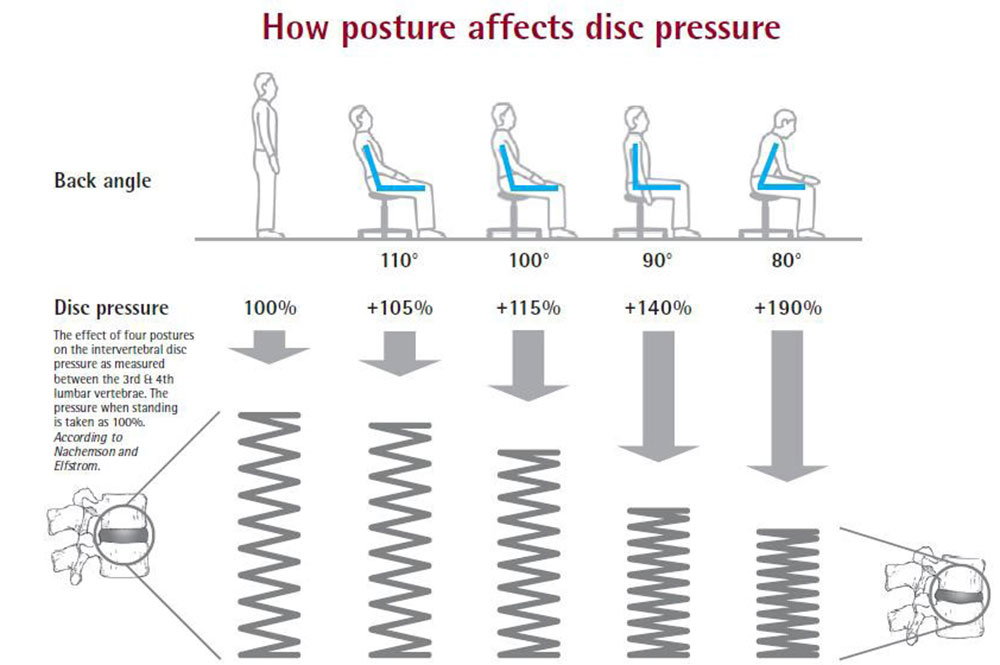
Sitting and Low Back Pain: The above diagram shows the relative disc pressures associated with different sitting postures.
References:
- Videman T, Nurminen M, Troup JDG. Lumbar spinal pathology in cadaveric material in relation to history of back pain, occupation, and physical loading. Spine. 1990; 15: 728-40.
- Hedman TP, Fernie GR. Mechanical response of the lumbar spine to seated postural loads. Spine. 1997; 22: 734-743.
5 Tips for Running Injury Free
With the arrival of Spring and some warmer weather more of us may be encouraged to venture outdoors to exercise. For most of us this may include running. Whether you are new to running or a well season runner follow theses tips from our physio Justin Merlino to help prevent common injuries associated with running and to keep yourself running injury free.
1. Effective Warm Up
There is some speculation as to what constitutes an effective warm up, but in my opinion it should involve a period of light aerobic activity to raise the core body temperature to the point of a light sweat, followed by dynamic stretching and then some sport/exercise specific drills. There has been some recent research that has shown dynamic stretching to be more effective than static stretching in preventing injury during exercise. Dynamic stretching might involve exercises such as gentle leg swings, calf raises, walking lunges, high knee running, hamstring kick-backs etc. This should be followed by some drills that are specific to the sport or exercise being undertaken. The entire warm up should take no longer than 30-45mins.
2. Avoid doing too much, too soon, too fast!
Any running program should be progressed gradually to allow the body to adapt to the training load. One of the most common mistakes in a running program is that the training volume and/or intensity is ramped up too fast, too soon. The body doesn’t have enough time to recover and adapt between training sessions and will ultimately result in overuse injury. A good running program should follow a step-like progression, with a gradual increase in training load over a 3-4 week period, followed by a lighter “recovery” week where the training load is slightly reduced. This 4-5 week cycle can be periodised into a full training program in the lead up to any major event or competition.
3. Recovery is key
It is probably the most important factor for preventing injuries and running injury free. Recovery is not only about cooling down and stretching after a training session, but it is also about hydration, nutrition, sleep and appropriate rest time between sessions. All of these components can be approached differently depending on the individual and the type of running being undertaken, but a good balance of all areas is essential in preventing injury.
4. Strength training
This can be a very effective tool for both improving running mechanics and preventing injury. An appropriate strength program can be developed by a health professional that targets specific weaknesses and biomechanical faults, helping to reduce the risk of future injury. Developing good body awareness and control is a great way to build the foundations for a healthy and long running career.
5. Listen to your body
Your body will shout out when an injury is lurking. Pain is the defense mechanism of the brain when there is the risk of bodily harm. Sometimes it’s difficult to know if the pain you’re feeling is just a slight niggle that will go away or if it is something that will turn into an injury. My advice is that if the pain is worsening throughout the session, if it’s altering the way you run, or if it’s above a 3 out of 10 ( 0 being no pain, 10 being excruciating pain) then you should cease running and let it rest for a few days. If it’s still sore on consecutive sessions then you should see a physiotherapist.
If you would like to book an appointment with Justin to discuss any of these tips or any pain you may be experiencing whilst running you can book an appointment with him either by calling (02) 8323 7777 or by clicking here.
What is Physiotherapy?
Physiotherapy Defined
Physiotherapy is a clinical health science and profession that aims to rehabilitate and improve people with movement disorders by using evidence-based, natural methods. “Physiotherapy can help recover from injury, reduce pain and stiffness, and increase mobility. A physiotherapist can also help you prevent further injury by listening to your needs and working with you to plan the most appropriate treatment for your condition, including setting goals and treatment outcomes.” (APA Website).
Watch this short film clip from the Australian Physiotherapy Association (APA) to see how physiotherapy could help you and your family return to your goals of work, activity and sport.
[youtube_video] CWDzA0pnaAY [/youtube_video]
What kind of treatment can I expect to receive?
Physiotherapists will create an individual treatment plan taking into account your everyday activities, lifestyle, work and sporting commitments. Treatments you can expect to receive as part of your plan may include;
- Tailored exercise programs to increase strength and improve mobility
- Joint manipulations to improve mobilisation and symptoms of pain and stiffness
- Breathing exercises
- Massage therapy to release muscle and soft tissue
- Dry needling
- Real time ultrasound
- Assistance with the use of walking boots, braces, casts and crutches
- Post-operative rehabilitation
What can I expect from a Sports Physiotherapist?
Sports physiotherapy focuses on the treatment, management, prevention and rehabilitation of injuries sustained during playing sports. Common sports injuries include bruises, strains and sprains, and joint injuries, caused by a direct blow or indirect force. Over-use injuries, such as stress fractures, are also a common sports injury.
Physiotherapy treatment will enable you to build strength, mobility, balance and co-ordination to overcome your injury and allow you to return to your sport safely and with the aim of avoiding re-injury.
For more information
Head to the APA website for more information on the physiotherapy profession. Remember a referral is not required to see a physiotherapist so for more information or to book a consultation call us on (02) 8323 7777 .